

Department of Pedodontics
The Department of Pediatric Dentistry was founded by Prof. Dr. Bora ALTINEL ATAMAN in 1963.
Pediatric dentistry is a branch of science that examines all kinds of oral and dental problems from the birth of the child to the adolescent age and produces solutions in cooperation with other branches of dentistry covering treatment and preventive applications. Until today, a total of 41 doctorates have been successfully completed their pHD in our department. Our department, which was established with three faculty members, has become a department with a respected and experienced staff of our faculty. We support international student exchange program at the internship level and still continue these activities within the scope of the ERASMUS program.
Our department has organized 2 national pedodontics congresses so far. In our department, undergraduate and graduate education and training programs, national and international scientific research and studies continue.
Health services applied in our department are:
-Preventive dentistry
-Fissure sealant application
-Restorative treatment for primary and permanent teeth
-Root canal treatment and vital pulp treatment for primary and permanent teeth
-Growth and development of jaws
-Space maintainers and prosthetic rehabilitation in children
-Preventive orthodontics
-Management of traumatic injuries to primary and permanent dentition
-Regenerative endodontic treatment
-Dental care for patients with special needs
-Dental treatment under sedation and general anesthesia
Academic Staff
International Dental Care
A)FLUORIDE
Cavities form when there is a weakening in the mineral composition of the enamel of your teeth. Fluoride promotes the remineralization of these decalcified spots, therefore helping to prevent cavities. Fluoride can also be found in many household products such as toothpaste, mouth rinses, and even some bottled water. Professional fluoride products should only be applied by or under the direction of a dentist or physician who is familiar with the child’s oral health and has completed a caries risk assessment.
Topical fluoride application is one of the most effective ways of preventing caries. . This can be achieved by frequent application of low concentrated fluoride solutions or preparations or less frequent application of high fluoride concentration preparations causing fluoride deposits in or on the enamel that will slowly be released to the plaque–enamel interface. As a general rule the fluoride should match the caries activity of the child, that is, the greater the cariogenic challenge, the more intense the fluoride treatment.
Fluoride-containing varnishes. Fluoride varnishes often contain high concentrations of fluoride and adhere to tooth surfaces for days, thus considerably increasing the fluoride content in the surface and subsurface enamel. The varnishes are easy to apply and two applications a year will give a good effect.
Fluoride gels are available on the market with different fluoride concentrations and tastes. They are mostly applied in custom-made trays and are used either in a professional setting or on a daily basis at home. Due to the risk of swallowing, they should not be used in preschool-aged children.
Fluoride toothpaste is the ideal vehicle to apply fluo- ride to teeth. Daily use of fluoride toothpaste will result in caries reductions of at least 20–40%.
 |
 |
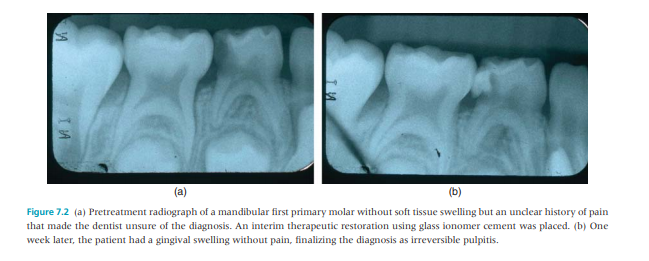
B) ATRAUMATIC RESTORATIVE TREATMENT
ART takes a position between nonoperative and restorative care, since the treatment consists of removing the superficial layer of carious dentin with only hand instru- ments and using a GIC as a combined restorative and sealing material. The ART technique is indi- cated primarily for treating single-surface cavities in both primary and permanent dentitions
 |
 |
C) EARLY CHILDHOOD CARIES
Early childhood caries (ECC) is usually seen in 18- to 36-month-old children, although it can present even younger. Initially, the maxillary incisors develop a band of dull white demineralization along the gum line that goes undetected by the parents. As the condition progresses, the white lesions develop into cavities that girdle the necks of the teeth in a brown or black collar. The premature loss or unsightly appearance of grossly decayed primary anterior teeth may be initially of concern to parents; however, as the child matures, it may also affect the patient’s self-image.
Treatment plans advocated for grossly decayed primary anterior teeth include the following: restorations, crowns, or extractions followed by partial dentures.
 |
WHY RESTORE PRIMARY TEETH?
Our child patients deserve the best dental treatment that clinicians can provide as any treatment – preventive or restorative – will shape their dental future. The objective of any restorative treatment is to:
- Repair or limit the damage of dental caries.
- Protect and preserve remaining the pulp and remaining tooth structure.
- Ensure adequate function.
- Restore aesthetics (where applicable).
- Provide ease in maintaining good oral hygiene.
In addition restoring primary teeth ensures that the natural spaces in the child’s primary dentition are retained for the developing permanent dentition.
In the primary dentition, dental restorations should ideally last until natural shedding of the tooth. However, the prognosis for a restoration in primary teeth is poorer than for those in the permanent teeth
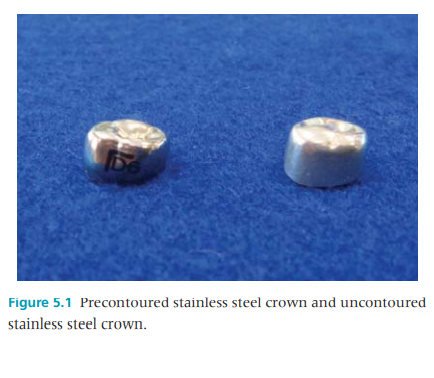
STAINLESS-STEEL CROWNS
Preformed stainless-steel crowns are available for most tooth types, both primary and permanent.
There are two major indications for use of such crowns in pediatric dentistry:
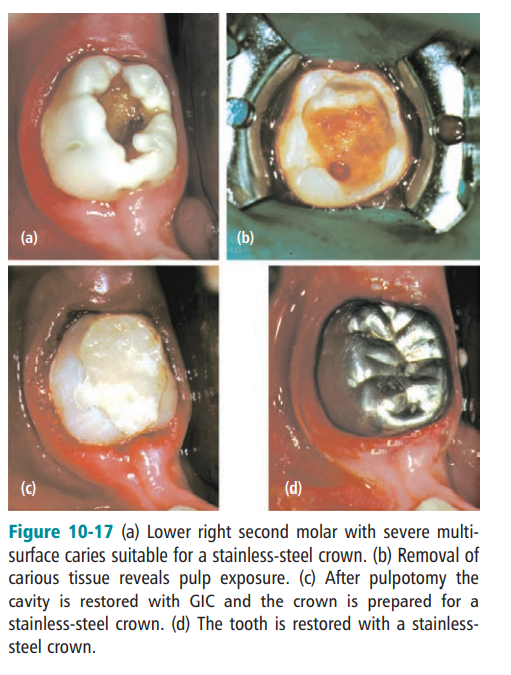
• Primary molars with extensive destruction of the crown
• Permanent first molars with severe developmental defects.
 |
 |
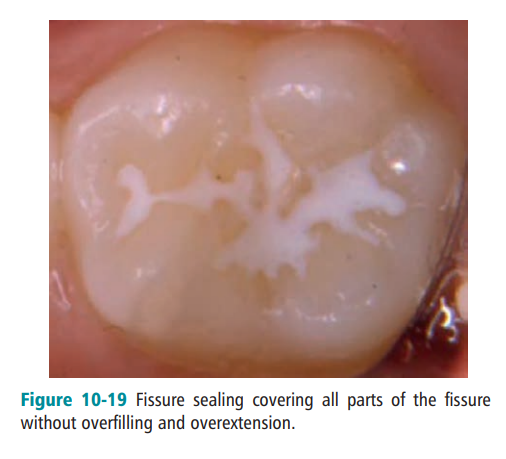
PIT AND FISSURE SEALANTS
Sealant materials may be transparent or opaque. Opaque materials are available in tooth color or white. Transparent sealants are clear, pink, or amber. The clear and tooth-colored sealants are esthetic but are difficult to detect at recall examinations.
The cariostatic properties of sealants are attributed to the physical obstruction of the pits and grooves. This prevents colonization of the pits and fissures with new bacteria and also prevents the penetration of ferment- able carbohydrates to any bacteria remaining in the pits and fissures, so that the remaining bacteria cannot produce acid in cariogenic concentration.
Sealants are thin, white plastic coatings that are applied to the tops or chewing surfaces of back teeth and are highly effective in preventing tooth decay. The naturally occurring pits and grooves on the chewing surfaces of teeth can often collect plaque. These small grooves and cracks are the most susceptible to cavities in children and teens and benefit the least from topical fluoride.
 |
SPACE MAINTAINERS
Primary teeth have many important roles in the health and development of children. Primary teeth are vital to chewing, speaking, smiling, aesthetics and holding space in the jaws for the developing permanent teeth.
Space maintainers are used when a primary tooth has been prematurely lost (or extracted) to hold space for the developing permanent tooth. If space is not maintained, teeth on either side of the extraction site can drift into the space and prevent the permanent tooth from erupting into its proper position. The space maintainer will be removed from your child’s mouth once his/her permanent tooth replacing the extracted tooth comes in.
 |
 |
PULP TREATMENT (PULPOTOMY)
Pulp therapy (pulpotomy) is the treatment of infected nerves and blood vessels in teeth. Pulp therapy generally becomes necessary for two reasons: either as a result of extensive tooth decay (dental cavities) or as the result of tooth injury.
Many cavities may be so deep that they extend to the nerve, often causing pain and discomfort. When this happens, the infected part of the nerve must be removed. The remaining healthy nerve will be left intact and medicated. The purpose of a pulpotomy is to extend the life of the baby tooth, thereby avoiding the need for extraction and a space maintainer, until the eruption of the permanent tooth.
 |
 |
EXTRACTIONS
Extractions are done only as a last resort in the case of severe tooth decay. If a primary molar is removed prematurely, a space maintainer will be placed. Some extractions are needed for orthodontic reasons to help facilitate tooth alignment when crowded teeth are present. Primary teeth are essential in maintaining the correct spacing in your child’s jaw for the permanent teeth.
 |
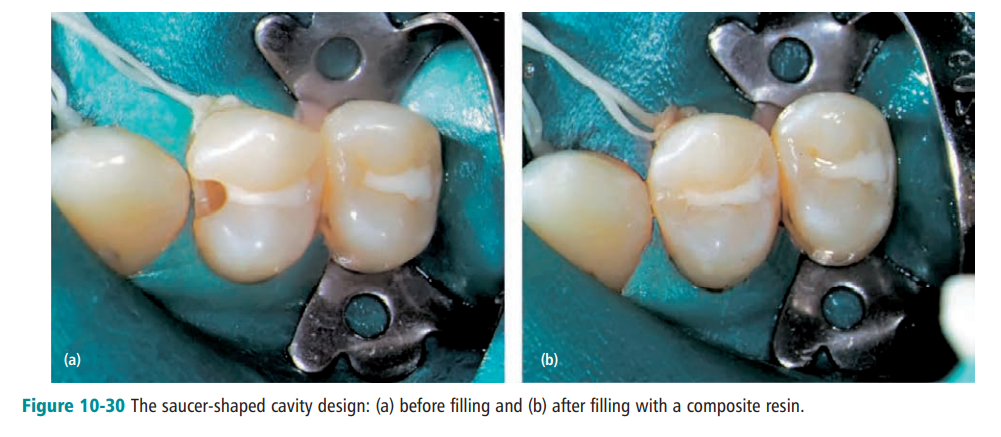
RESTORATIVE MATERIALS
The restoration of carious lesions in primary and young permanent teeth to be among the important services that pediatric dentists.
Injuries to the teeth of children or adults present unique problems in diagnosis and treatment. The diagnosis of the extent of the injury after a blow to a tooth, regardless of loss of tooth structure, is difficult and often inconclusive. Trauma to a tooth is invariably followed by pulpal hyperemia, the extent of which cannot always be determined by available diagnostic methods. Congestion and alteration in the blood flow in the pulp may be sufficient to initiate irreversible degenerative changes, which over time can cause pulpal necrosis. In addition, the apical vessels may have been severed or damaged enough to interfere with the normal reparative process. Treatment of injuries causing pulp exposure or tooth displacement are particularly challenging, because the prognosis of the involved tooth is often uncertain.
The treatment of fractured teeth, particularly in young patients, is further complicated by the often difficult but extremely important restorative procedure. Often the likelihood of success depends on the rapidity with which the tooth is treated after the injury, regardless of whether the procedure involves protecting a large area of exposed dentin or treating a vital pulp exposure. Several factors can be considered common to all types of injury to the anterior teeth.
 |
 |
B) DEPARTMENT OF PEDIATRIC DENTISTRY
Division of Clinical Sciences contains Oral and Maxillofacial Surgery, Oral and Maxillofacial Radiology, Operative Dentistry, Endodontics, Orthodontics, Pediatric Dentistry, Periodontology, Prosthodontics Departments in itself. The Departments runs patient services and licence education programme. In addition, Departments conducting scientific researches and runs postgraduate education programmes





